Ligation of
Arteries During the Civil War
By Dr. Michael Echols
Edited from the medical textbook
Handbook of Surgical Operations,
U. S. A. Medical Department, 1863,
(in this collection) written during the Civil War by
Stephen Smith,
M.D.
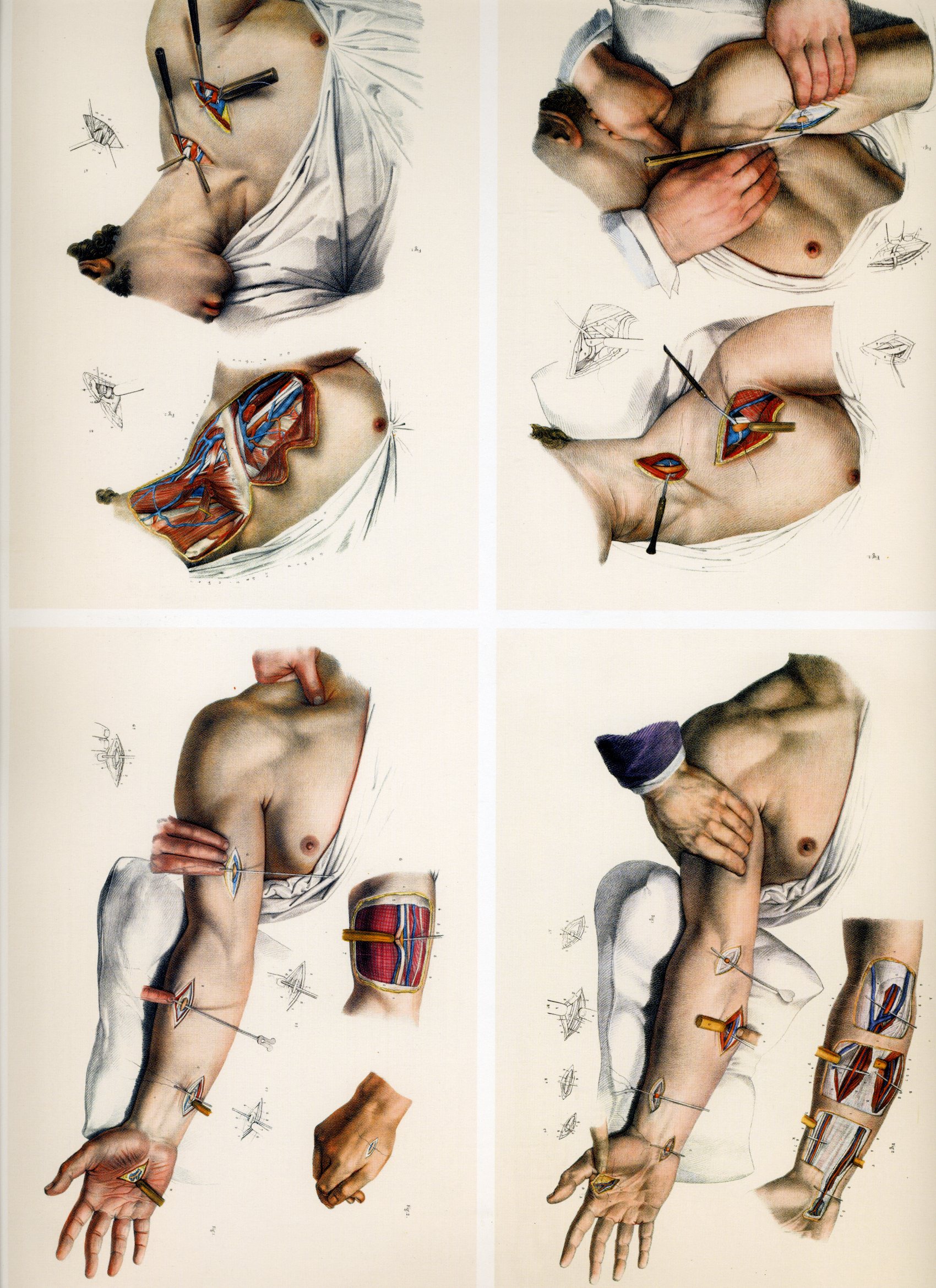
Civil War medicine diagrams from Bourgery & Jocob.
LIGATION OF ARTERIES
The object sought in the ligation of
an artery is the permanent obstruction of the current of blood by the
obliteration of its cavity. To effect this object the internal coats of
the vessel should be ruptured by the ligature; the process of
obliteration then consists in the organization of the clot in the vessel
with the adhesion of the ruptured tunics.
Instruments: The instruments
immediately required are a scalpel, forceps, aneurismal needle,
ligature, director, and spatulas.
The Scalpel: The common scalpel
answers the best purpose in this operation. Its blunt, rounded edge, is
best adapted to the dissection, and the broad extremity of the handle
can be used to advantage in separating layers of fascia, and parts where
the cutting edge is not desirable.

The Forceps: The common
dissecting forceps should be selected for the dissection; they should
have accurately fitting teeth, and not be liable to open at the
extremity when firmly closed; a pair of small forceps may also be
required.

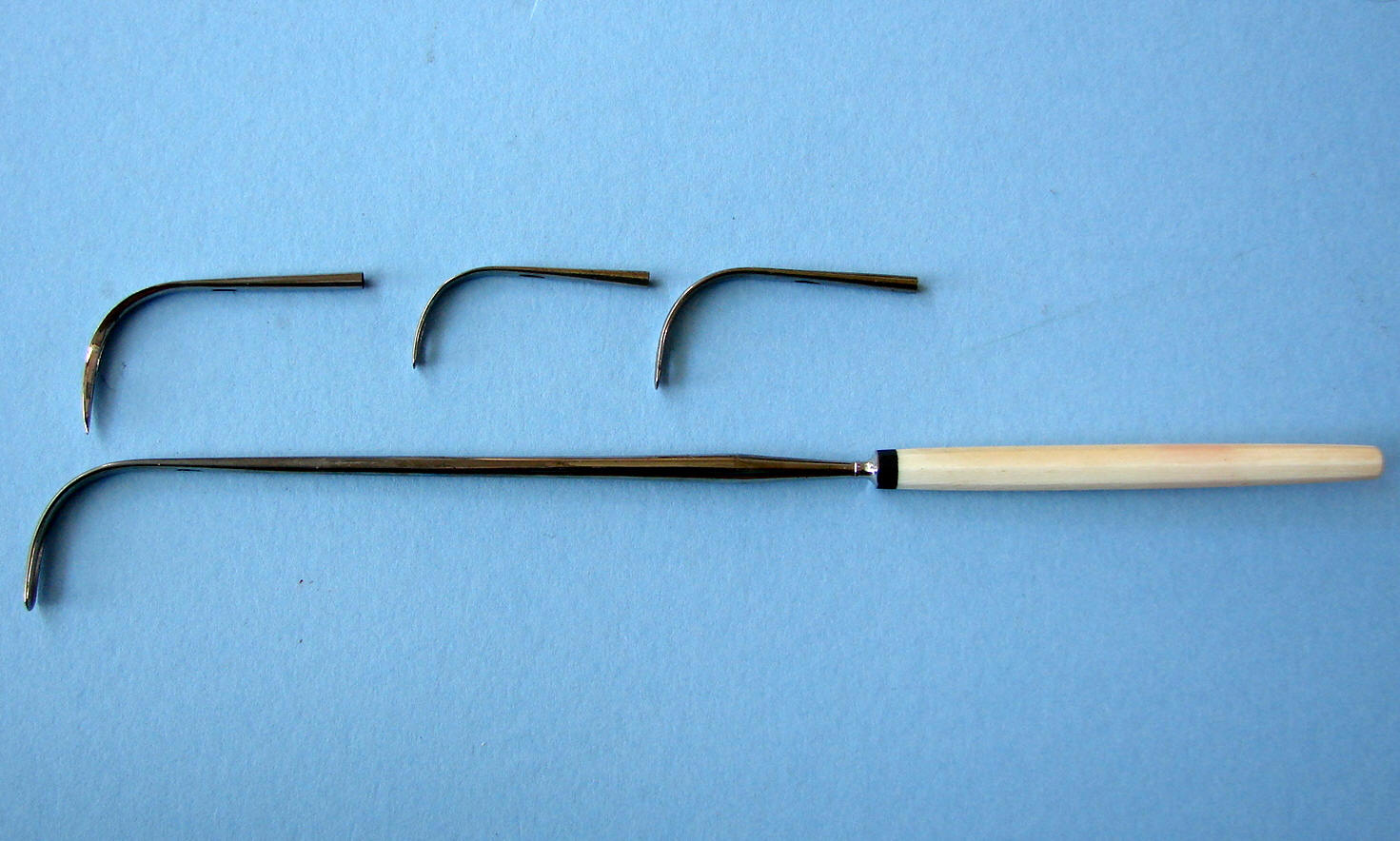
The Needle: The common
aneurism needle is a curved blunt instrument, with an eye near the
extremity, and firmly fixed in a handle (Fig. 51). When used, the
extremity is gently insinuated under the vessel, and as it appears upon
the opposite side, the loop of the ligature is seized with the forceps,
or a hook, and one end being drawn through, it is held as the instrument
is withdrawn, carrying the other end, and thus leaving the ligature
under the vessel. Of the different needles invented for this operation,
that known as the " American needle," of Dr. Mott, is, perhaps, the most
convenient, and is especially well adapted to those cases where the
artery lies very deeply. It consists of the handle and hook
and the blunt needle with two eyes .
|

Mott's "American" aneurism suture set with removable
screw mounted tips as found in a typical Civil War
surgical set
|
 |
The needle is fitted to the shank by a screw
mount. When used, the ligature is first inserted into the second eye;
the needle is then passed under the artery, and as the extremity emerges
upon the opposite side, the hook is inserted into the eye, and the needle
is thus held until the
handle is unscrewed, when it. is drawn through with the ligature. It is
sometimes necessary to include other tissues with the artery, when the
sharp-pointed needle is used.
The Director. The director is
used in the dissection to raise the fascia before its division; it is
sometimes passed under the artery as a guide to the needle.

Spatulas. Two spatulas are
often required, with which assistants separate the sides of the wound,
and expose the deep- seated parts; pieces of flexible metal or wood may
be used.

The Ligature. The ligature is
generally of the strongest dentists' silk, or of silver wire; its size
proportionate to the size of the vessel.

Arrangements. The patient is placed
upon a firm bed or on a table, and the assistant administers the anaesthetic; the surgeon takes his position generally on the outside of
the limb which is the seat of the operation; a second assistant takes a
position where he-can command the artery above if by any accident it is
wounded, or if the artery yields under the tightened ligature; a third
uses the sponges; and a fourth separates the wound with the spatulas.
Position of the Artery. The
precise location of the artery is determined, 1. By its pulsations; 2.
By given anatomical points in the vicinity. To render the former
distinct, the limb should be placed in a position favorable ' to
arterial circulation; to render muscles and tendons most
distinct the limb should be forcibly extended at the commencement of the
operation. When the dissection has proceeded so far as to reach the
vicinity of the artery, the operator is aided in detecting its position
by flexing the limb so as to relax the muscles and tissues.
Position of Superficial Veins. It
is important, before the first incision is made, to guard against
wounding superficial veins. Their position is readily defined by
compressing the parts above the point of the proposed operation.
|

|
|
Drawings from Bourgery & Jacob
|
Operative Procedure. The operation
involves several consecutive steps: Incision: When the first
incision is about to be made, the skin should be rendered tense by the
thumb and fingers of the left hand applied on either side of the vessel,
or the fingers applied at the extremity of the proposed incision,
parallel to its course; if the first method is chosen, care must be
taken not to make more traction on one side than on the other; the
second method answers where the skin is naturally tense and but slight
traction is necessary.
The scalpel should be held in the
second or third position, and the incision should be
made directly over and generally parallel to the artery, through the
skin only if the artery is superficial, but also through the
cellular tissues if it is deep, ita length varying with the depth of
the vessel and the fleshiness of the subject. The incision is
sometimes made in the direction of the fibres of the muscle covering
the artery, as where the great pectoral overlies the axiliary; at
other times it should be curved, so as to raise a flap. The length
of the incision cannot be prescribed, but it should always be ample.
Dissection of Fascice and
Muscles: The fasciae are carefully pinched up with the forceps, and being opened with the scalpel applied horizontally,
are incised freely on a director introduced beneath them. In
dissecting among muscular structures it is important to enter the
muscular interstices, and not wound the substance. These
inter-muscular spaces are marked by deposits of fat, especially
towards the terminal extremity of the muscles, and hence we should
commence the separation of muscles as nearly as possible at their
terminal extremity. If there is doubt as to the line of separation,
a puncture with the bistoury will disclose adipose or muscular
tissue, according to the nature of the underlying structure. If the
dissection is made through the body of the muscle, the fibres
separate more readily in an inverse direction, viz. from their
origin to their attachments. The muscles may be separated with the
handle of the scalpel or the finger nail.
Isolation of the Artery: The
larger arteries have firm sheaths, which require to be opened by
dissection; the smaller vessels have but slight fibrous investments,
and are readily exposed with the point of a director, or the
aneurism needle. The true sheath of the artery is opened by pinching
up a small portion with the forceps, and nicking it slightly with
the scalpel, held as before noticed; into the opening
thus made, the end of a director or the aneurism needle is gently
insinuated, and by slight movements of its point, first upon one
side and then upon the other, the sheath is separated completely
around the vessel, to an extent sufficient to allow simply the
passage of the ligature; as the extremity of the instrument emerges
on the opposite side, the finger of the left hand, or the thumb and
forefinger pressed together, should steady its point as it
penetrates the last of the investing sheath.
Passage of the Ligature.—If
the artery is small and very superficial, a director may be passed
under, and along its groove a blunt needle carrying the ligature. If
more deeply situated-the common aneurism needle or the American
needle should be used.
|